
By Herb Townsend
My Running History
You might say that I’ve been an avid runner for most of my 84 years. In a quest for improved fitness, I began running in 1977 at age 39 by entering a 9.8-mile race. That experience got me hooked on distance racing. Since then, I have logged over 130,000 total running miles, and competed in thousands of races, including 75 marathons, 1 ultra marathon, 4 triathlons, and 7 duathlons. Although I was never close to being an elite runner, I was usually competitive in my age group, and was able to set numerous age-group course records. My personal best marathon (2:40:42) occurred in 1984 at Philadelphia. But my most cherished memory was being the overall winner of the Great Valley Marathon in Chambersburg, PA in 1990 at age 51 in a time of 2:51:39. Despite these accomplishments, there was always an underlying feeling that I might have done better if I started running at an earlier age, and hadn’t spent my teen years and early 20s smoking, drinking, and working on motor bikes and cars. In any event, becoming a runner has allowed me to meet many great people, and took me to many places in the world that I would not otherwise have seen. And, until recently, I believed that it also kept me fit and healthy.
Declining Performance with Age
Over the past few years, my race performances have steadily declined. Obviously, much of this can be attributed to the inevitable effects of aging. But more recently, it seemed to be something more than just old age. Whereas in my mid-forties, my age-graded race scores were generally in the range of 80-89%, by the age of 83, they had sunk to the 59-62% range.
Diagnosis — Aortic Valve Stenosis (AVS)
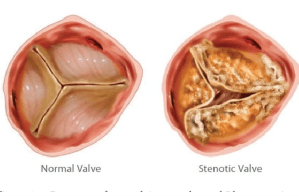
The next clue that something more than normal aging was occurring came during my annual wellness checkup. The examining doctor didn’t like the sound of my heart, so he sent me for an echocardiogram, a test that shows ultrasonic images of the beating heart. Those images revealed a condition that was labeled aortic valve stenosis (AVS).
I soon learned that my AVS was the result of “calcium deposits” on the aortic valve. The term “calcium deposit” is a simplified description of atherosclerotic plaque, a mixture of fats and the mineral calcium hydroxy appetite, which deposits on the inside surface of arteries as we age. Because calcium components can be readily detected by x-ray analysis, the amount of plaque is often quantified in terms of the amount of calcium. When these deposits are formed on the flaps of the aortic valve, they reduce the ability of this valve to fully open, thus reducing the flow of oxygenated blood from the lungs through the heart to the rest of the body.
Particularly alarming were statements I found online, such as: “The average overall survival rate is two to three years in symptomatic patients without surgical treatment,” and data showing that the 5-year survival rate for severe AVS was less than that of metastatic lung, breast, ovarian, prostate, and colorectal cancers. My reaction to this news was a mixture of surprise, disbelief, and confusion. How could someone who engages in daily, vigorous exercise, and has been careful with diet, develop a serious heart condition? After the initial denial came the inevitable acceptance when I realized that the AVS diagnosis may have provided a reason for my greater-than-expected loss of speed. It was also comforting to learn that the condition can treated.
Treatment of AVS
Ai this time, there is no accepted way to remove calcium deposits from heart valves. There is a group in Europe looking at insertion of an ultrasonic probe through a catheter directly to into the heart to scour away calcium deposits from the valve. But realistically, it will be many years, if ever, before this method is widely available. So, in general, AVS is currently treated by replacing the old, calcified valve with a new, artificial valve.
In the past, valve replacement meant that a surgeon would have to split open the chest to gain access to the heart, remove the old valve, and replace it with an artificial one. Recovery from the trauma of open-chest surgery is both painful and slow, with a significant risk of infection and other complications. Fortunately, the development of a new technique, known as transcatheter aortic valve replacement (TAVR), avoids the need for open heart surgery. In the less-invasive TAVR procedure, a new valve is placed in the heart by use of a catheter inserted through an artery, usually from a femoral artery in the groin. With this method, there is less trauma, and recovery is much faster.
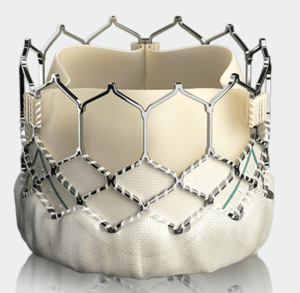
My TAVR surgeon uses a replacement valve assembly in which the actual working valve is made of cow tissue. The tissue is supported by a metal mesh frame (a cobalt-chromium-tungsten-nickel alloy) and a plastic (polyethylene terephthalate) skirt. Prior to insertion, the valve assembly is collapsed to allow it to fit within the catheter. Once the new valve is positioned in the heart within the old valve, it is expanded. The expansion crushes the old valve against the surrounding tissue, and holds the new valve in place.
Preparation Prior to TAVR
In advance of my TAVR, hospital trips for two tests were required. The first of these was a computerized tomography (CT) scan which gives a 3-dimensional image of the heart, thus allowing measurements to determine the size of the replacement valve. After being wired up for a simultaneous electrocardiogram, and having an IV inserted in my arm, I was run through the CT scanner. Next, a contrast-enhancing dye was injected via the IV, and I was CT scanned a second time. The entire procedure was painless, and took less than 15 minutes.
The second required test was a cardiac catheterization, also known as an angiogram.
This procedure consisted of inserting a catheter through my right wrist into my arteries and heart. This enabled injection of a dye to facilitate x-ray images of the aorta valve and heart interior. This test was also painless, and also took less than 15 minutes, although I was in the hospital for a total of 9 hours for various prep and post-op activities, but mostly just waiting for things to occur. The good news was that, although calcification of the aorta valve was confirmed, no blockages or structural abnormalities were detected.
Pre-TAVR Concerns
Prior to the TAVR, I googled as much information as I could about it. In addition to the usual surgical risks such as infection, bleeding, and death, one item of particular concern that stood out. One report stated that, in a significant number (9 to 26%) of TAVR procedures, the electrical signals that control the heartbeat are impaired. When this happens, permanent implantation of a pacemaker in the chest is needed to keep the heart beating properly. The thought of having a pacemaker in my chest for the rest of my life became a major worry. Nevertheless, a 26%-or-less chance of needing a pacemaker seemed like a better bet that than death in 2-3 years.
The TAVR Operation
Prior to the going to the operating room, I was put on a gurney in a holding area while a nursing crew prepared me for the event. Preparation included attaching numerous wires all over my body with adhesive to continuously monitor heartbeat, and inserting four intravenous ports, two each arm, to allow periodic injection of antibiotics, drugs, and fluids, as well as for withdraw of blood samples for analysis. It also included shaving my groin to facilitate catheter insertion. At that point I first learned that two catheters, one in each side, will be used for the implanting the new valve. The next surprise took place when they also shaved my chest, just in case the transcatheter operation went wrong making it necessary to open the chest cavity. This was as close as I came to panic.
After being prepped, I was wheeled though the hospital corridors to the actual operating room, a brightly lit place filled with a lot of machines and video displays. What seemed like at least a half dozen nurses and attendants worked quickly to move me from the gurney to the operating table, attach the IV lines to my ports, and plug in the electrical wires into the video monitors. The last thing I remember was someone putting a mask over my face and saying I was about to get some oxygen.
After about an hour, I woke up back in the prep area. The good news was that the operation was a success, and that I will not require a pacemaker. The not-so-good news is that I must remain overnight in the hospital, and that when I am lying in bed, I must remain on my back with my legs straight. I am also told that I will need to take Plavix (an anti-clotting agent) for the next 6 months, and aspirin (a blood thinner) forever.
First Months After TAVR
On days 1 to 5 after TAVR, I am walking 2-3 miles per day. I am disappointed because I don’t feel any better than I did prior to the operation. Even more concerning is that my resting pulse rate and blood pressure are higher.
By Day 5, I am beginning to feel better. My blood pressure and pulse rate are now almost normal, and I increase the speed of my walk, and mix in runs 20-second segments of running for a total of 180 seconds.
On Day 6, I meet with the cardiac-team nurse for my 1- week post-op checkup. My blood pressure and pulse are high again. The nurse does an EKG, and sees an irregularity in my heartbeat. I am told to wear a heart monitor so that the heartbeat can be monitored remotely for 7 days. I get the feeling that this could mean that I still might need a pacemaker, depending on the results. Otherwise, I feel pretty good and work out with free weights.
On Day 7, I am Feeling OK, and ran a bit faster. My blood pressure looked great, and pulse is coming down. The wireless heart monitor is installed and it is intended to remain in place for 7 days, except when it is removed for showering. Unfortunately, the heart monitor is attached to my chest with adhesive patches that fail to hold on while I am sleeping or running. Each time the monitor falls off, I reattach it with fresh adhesive patches, and hope that these interruptions periodic interruptions do not invalidate the results.
Day 15 is the last day for the heart monitor, and the first day that the monitor didn’t fall off, probably because it was cooler.
On Day 16, maybe it’s the mild weather, or that I resumed drinking regular coffee instead of decaf, but I’m finally feeling pretty good. Did a five-mile run with 8 X 200 speedwork. Even began thinking about registering for a 5K race on Sunday.
On Day 19, I ran a 5K race. At the starting line, my main concern was being able to finish without incident. My time was the worst ever for the distance (43:37 compared to 36:24 in the same race last year). It is now abundantly clear that the new valve did not produce any immediate miracles.
On Day 35, I do another 5K, this time in 36:37, almost as good as my last pre-TAVR time.
On Day 39, I get my one-month post-op checkup with the TAVR doctor. He tells me everything looks good, and the monitor-results confirm that I will not need a pacemaker. I can now look forward to a return to normality.
Categories: Features

Fantastic, Herb! Good luck.
LikeLike
TERRIFIC piece, Herb. At 76, my story parallels yours (except for speed & # of road races)- Running/jogging for 60+ years. Diagnosis- a year or so ago- Aortic Valve issue. 1st consult today with the surgeon to discuss open heart vs TAVR (leaning in that direction). Will have CT Scan & Angiogram done in 1/2023- than it’s decision time (hopeful TAVR will be the winner). I’m hoping my recovery will (at the least) match yours. Now I can relate to the pros & cons & post surgery situations from one who has been there & done that!
Best of Luck to you & hope to keep “pounding the pavement” a little quicker than I have been..
Jay
LikeLike
Thanks for your comment, Jay, and all the best to you!!
LikeLike
Hi Herb:
MISSION ACCOMPLISHED!
Angiogram completed on 2/2/2023- found 100% blockage in the left anterior descending artery (LAD)- Surgeon Roto -Rootered it out. TAVR completed 2/7/2023- 1.5 hrs- no issues- no pacemaker. Only soreness from the two groin entries to insert the TAVR (normal process & results). Began walking today (about a mile)- no jogging for a week.Feel GREAT!
Hope to resume some road races & snow skiing before long!
Hope all is well with you & you’re setting new records!
Jay
LikeLike